















 11 / 15
11 / 15

Page 32
J u l y 2 3 - 2 4 , 2 0 1 8 | R o m e , I t a l y
allied
academies
Joint Event on
Cardiology Congress 2018 & Microbe Infection 2018
Biomedical Research
|
ISSN: 0976-1683
|
Volume 29
2
nd
World Congress on
CARDIOLOGY
MICROBIOLOGY AND MICROBIAL INFECTION
&
39
th
Annual Congress on
Shyam K Ashok, Biomed Res 2018, Volume 29 | DOI: 10.4066/biomedicalresearch-C1-002
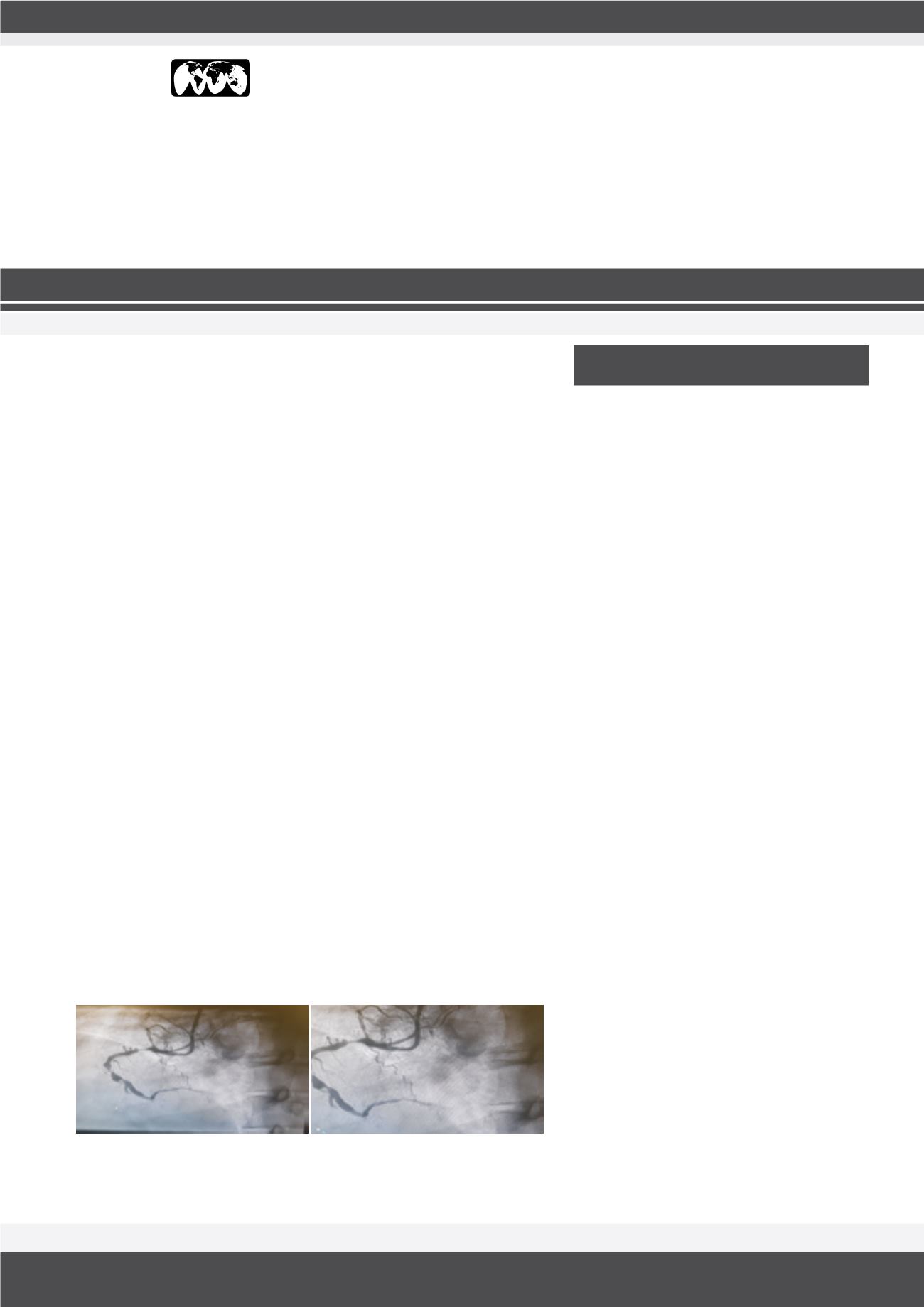
CABG IN DIFFUSE CORONARY ARTERY
DISEASE
Shyam K Ashok
Aster CMI Hospital, India
Statement of the Problem:
In India 2.78million death are due to cardiovascular
diseases of which 50% are due to CAD. Peculiarities of CAD patterns in Indian
patients- Younger age at presentation, high incidence of DVD and TVD, diffuse
involvement, distal disease and significant LV dysfunction at presentation.
Diffuse CAD: Length of significant stenosis >20 mm, multiple significant
stenosis (>70% narrowing) in the same artery separated by segment of
apparently normal vessel and significant narrowing involving the whole length
of coronary artery.
Methodology:
We in our institute, perform OP CAB and use LIMA and veins
as conduits to perform the surgery. Once the conduits are harvested, we
heparinize with I.V. Heparin 3 mg/Kg given to achieve an ACT >300. Using
the octopus as stabilizer, we perform an endarterectomy of the LAD first and
then use a vein patch to cover the defect. LIMA is then used to anastomose
the LAD on the vein patch. Veins are used to bypass the LCX and RCA, as
deemed appropriate. The proximal ends of the vein grafts are anastomosed
to Ascending Aorta with side clamp and heart beating. Intra op we start
Lomodex infusion 20 ml/hr which is continued for 24 hours and the inotropes
used are adrenaline and dobutamine as and when necessary. Postoperatively
aspirin 75 mg is given, and heparin infusion started after six hours to maintain
ACT of around 150 for 24 hours. Patients are usually extubated after four
hours provided they are hemodynamically stable. Anticoagulation by acitrom
is commenced orally fromday one tomaintain an INR of two for threemonths.
Result:
Out of the 20 patients in last 18months outcomes have been excellent
with no in-hospital mortality or cerebrovascular incidents.
Conclusion:
Off pump CABG with coronary end-arterectomy offers a good
solution to the problem of diffuse coronary artery disease.
Shyam K Ashok after completing his MBBS and MS
in General Surgery, he did his MCh in CVTS from Seth
GS Medical College, Mumbai in 2008. He later joined
Narayana Hrudayalaya, Bangalore in 2008, which is
a 1000 bedded hospital executing close to 600 open
heart surgeries in a month. He worked as a Fellow in
Adult Cardiothoracic Department in Royal Melbourne
Hospital, Australia, which is the second largest cardio-
thoracic unit in the whole of Australia. After working
in Australia for two years he re-joined Narayana Hru-
dayalaya, as Consultant Cardiothoracic Surgeon in
2012, and worked there till 2015. He has independent-
ly performed about 1000 open heart surgeries, con-
sisting of coronary artery bypass surgeries and valve
replacements. His area of interest is coronary artery
bypass, especially total arterial revascularization. He
joined Aster CMI Hospital in Feb 2016, as Consultant
Cardiothoracic Surgeon.
shyams2u@yahoo.co.ukBIOGRAPHY