













 2 / 6
2 / 6

Page 12
allied
academies
Curr Trend Cardiol. 2017 | Volume 1 Issue 3
September 18-19, 2017 | Toronto, Canada
Annual Conference on
HEART DISEASES
Notes:
Introduction:
The holy grail of the prevention of
atherothrombotic disease (ATD) lies with the prediction of
the population at risk of ATD. Many different risk predictors
have been advocated, but none universally accepted. The
author presents his risk predictor based on the characteristics
of those who have developed some form of clinical ATD
during the 4November 1974-4November2003 time frame.
Purpose:
Following the precepts of the Framingham Heart
Study, the author has analyzed the constellation of ATD
risk factors that characterize the ATD population and has
generated a predictive tool that accurately characterizes that
population.
Methods:
The author has examined his patient population
database and separated out those who developed some
form of clinical ATD during the study timeframe, compared
with those who did not.
Results:
The population who developed ATD is characterized
by cigarette smoking, dyslipidemia, and (often) hypertension,
with some contribution from uncontrolled diabetes. ATD
patients are defined by an abnormal lipid ratio, as defined
by the Cholesterol Retention Fraction (CRF, defined as
[LDL-HDL]/LDL) with/without cigarette smoking and/or
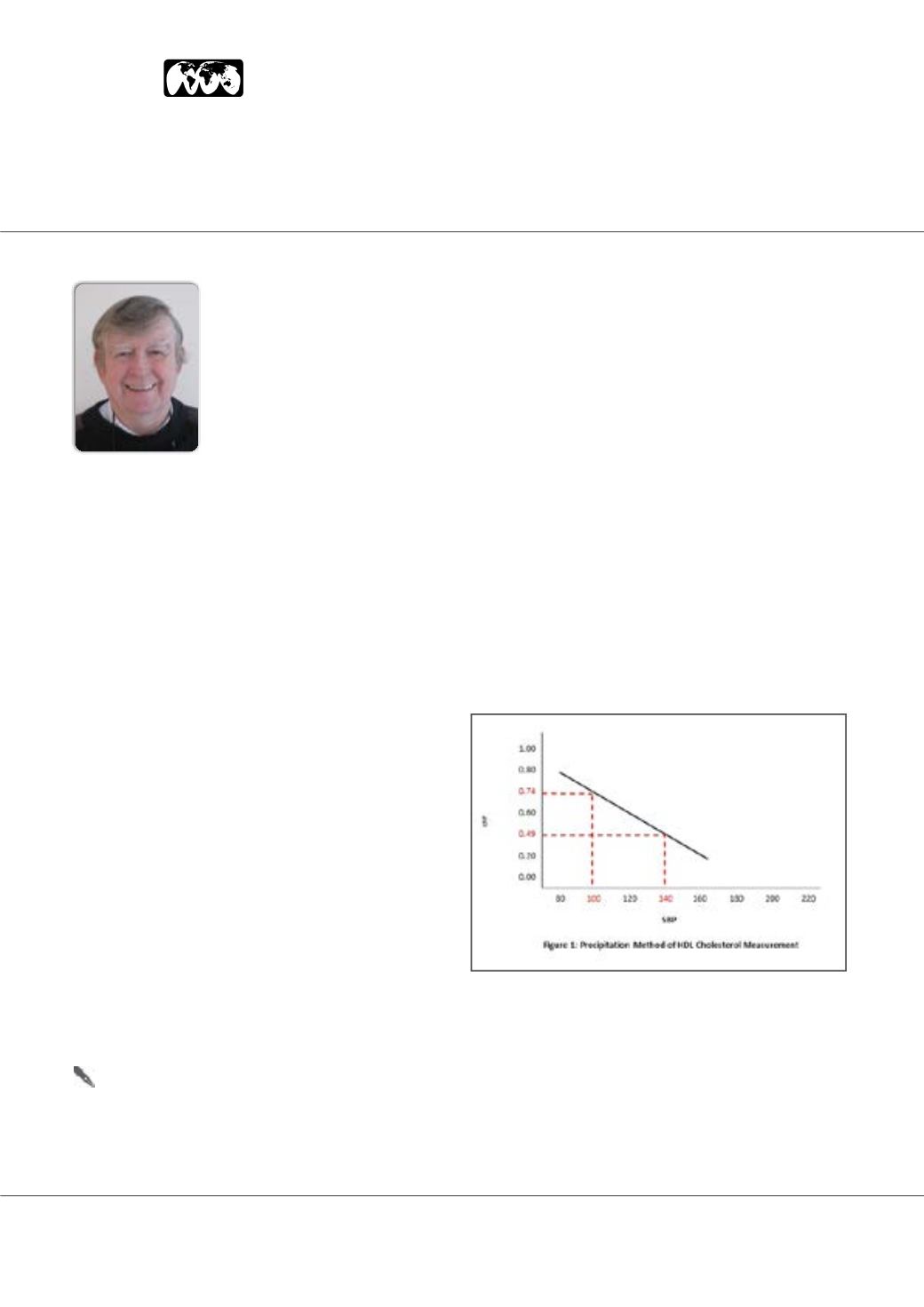
hypertension. This is best seen in a risk factor graph with
the CRF on the ordinate and systolic blood pressure (SBP).
The graph is characterized by a threshold line with CRF-SBP
co-ordinates (0,74,100) and (0.49,140), above which lie the
CRF-SBP plots of 93% of all of the ATD patients (710 patients)
in the author’s practice (See Figure.1). Fine tuning of risk
prediction is done by stratification by cigarette smoking
status, and the outcomes of the ATD patients are given in
Table I. Additional risk stratification is done by stratifying
CRF vs SBP and CRF by LDL-cholesterol. Any therapy that
brings the CRF-SBP plot below the threshold line results in
plaque stabilization/regression in a minimum average of 76%
of cases.
Conclusions:
The population at risk of ATD is predictable and
hence preventable.
William E Feeman
Bowling Green Study, USA
Enhanced prediction of the population at risk of atherothrombotic disease