- Biomedical Research (2010) Volume 21, Issue 4
Case Report- Gorlin Goltz Syndrome (GGS) - Report of a rare case
Farzan Rahman1, Shoaib R Tippu2 , RM Vatchala R3, KL Girish4, K Umesh51Department of Oral and Maxillofacial Pathology, Jaipur Dental College, Jaipur, India.
2Department of Oral and Maxillofacial Surgery, Jaipur Dental College, Jaipur, India.
3Department of Oral and Maxillofacial Pathology, Jaipur Dental College, Jaipur. India.
4Department of Oral and Maxillofacial Pathology, Jaipur Dental College, Jaipur. India.
5Principal, Al Ameen Dental College, Bijapur. India.
- *Corresponding Author:
- Farzan Rahman
516, Unique Sanghi Appartments
Mahaveer Nagar
Jaipur 302016.
Phone: +919783033999
E-mail: drfarza@hotmail.com
Accepted date: March 21 2010
Abstract
Gorlin's Goltz syndrome (GGS) is a rare autosomal dominant inherited condition. It in-volves many organs, but principally affects the skin, skeleton, endocrine and nervous sys-tems. It consists of the classic triad of basal cell carcinomas, multiple jaw cysts and skeletal deformities along with other defects. The authors report an unusual case of a fifteen year old male patient who reported with the complaint of swelling and mild pain in the lower right side of the jaw. Investigations revealed multiple cystic lesions in both upper and lower jaws which were found to be Odotogenic Keratocysts (OKC), presence of bifid rib and mul-tiple nevi. The clinico-pathological diagnosis was made as Gorlin- Goltz syndrome (GGS) since the present case exhibited three major criterias.
Keywords
Nevoid basal cell carcinoma syndrome, Gorlin Goltz syndrome, Bifid ribs, Multiple odontogenic keratocyst cysts, Multiple Nevi, Palmar pits, PTCH gene.
Introduction
Gorlin-Goltz syndrome (GGS) is a rare autosomal domi-nant disorder that involves multiple organ systems, in-cluding the skin, skeleton and jaws. Odontogenic kerato-cysts. bifid ribs and nevoid basal cell carcinomas are the hallmark of the disease.[1-4] Jarisch White in 1894 first reported regarding the association of nevoid basal cell carcinoma with skeletal anomalies as cited by Fitz Patrick PJ.[2] It was in 1960, Gorlin and Goltz established a clas-sical triad that characterises the diagnosis of this syn-drome which included multiple basal cell carcinomas, keratocysts in the jaws and bifid ribs and hence the name.[3] We present a rare case of Gorlin Goltz syn-drome.
Case Report
A male patient aged 15 years reported to clinics of Jaipur Dental College, Jaipur, with a complaint of swelling on the right lower jaw since one year. The swelling slowly progressed to the present state which the patient noticed only when visible facial asymmetry occurred.
On extra oral examination there was facial asymmetry because of a solitary diffuse swelling on the right side of the face involving middle and lower third region of the face (Figure 1). Intra oral examination revealed that the buccal and lingual vestibule in relation to 44 to 47 was obliterated with diffuse swelling (Figure 2). A thorough oral examination also revealed missing 32, 33, 34 and 35 and retained 74 and 75. Orthopantomograph (OPG) was advised to arrive at a final diagnosis. The OPG revealed multiple multilocular radiolucencies in relation to 47 and 48 and also in relation to impacted 32, 33, 34 and 35. Unilocular radiolucency was also observed in relation to erupting 18, 28 and 38 (Figure 3).

Figure 1: Photograph showing facial asymme-try and multiple nevi on face and neck.

Figure 2: Intra-oral photograph showing lingual swelling in relation to mandibular poste-rior region.

Figure 3: Orthopantogram showing multiple cystic lesions.
Then out of suspicion, face and other parts of the body were thoroughly examined which revealed multiple nevi on the face, neck and back region (Figure 1). It was de-cided to go for a chest radiograph as he exhibited pigeon shaped chest (Figure 4). The chest radiograph confirmed the presence of bifid ribs (Figure 5). His hands and feet were searched for any palmar and plantar pits which were not found. CT scan was advised for proper treatment planning. The findings of the CT scan revealed multiple cystic lesions in both the jaws.

Figure 5: Chest X-ray showing Bifid rib (circled).
Surgical treatment with enucleation of all cystic lesions was done under general anaesthesia with peripheral ostec-tomy and chemical cauterisation with Carnoy’s solution (Figure 6). All the five samples of the cystic lesions along with the involved teeth were sent for detailed histopathological investigations to Department of Oral Pathol-ogy (Figure 7). Based on the histological features it was diagnosed as Odotogenic Keratocyst (Figure 8). Similarly other two specimens were also diagnosed as infected Odotogenic Keratocyst with daughter cyst, one with Odontogenic Keratocyst and Dentigerous cyst. Correlat-ing with the clinical, radiographic and histo-pathological features, it was diagnosed as Gorlin Goltz syndrome.

Figure 6: Intra-operative photograph showing cyst enucleation.

Figure 7: Gross appearance of all the cystic lesions.

Figure 8a: Photomicrograph of OKC showing cystic lumen lined by conjugated parakeratinized epithelial lining and capsule (H & E staining 4x).

Figure 8b: Photomicrograph of OKC showing corrugated parakeratinized epithelial lining and seperation from the capsule (H & E staining 20x).
Discussion
Gorlin-Goltz syndrome is an autosomal dominant inher-ited disorder with high penetrance and variable phenotype expressiveness which can manifest itself spontane-ously.[4,5] It is characterized by the development of multi-ple odontogenic keratocysts, frequently beginning in the second decade of life, and or basal cell carcinomas (BCCs) usually from the third decade onwards. Approximately 60% of individuals have a recognizable appear-ance with macrocephaly, bossing of the forehead, coarse facial features, and facial milia.
Most individuals have skeletal anomalies (e.g., bifid ribs, wedge-shaped vertebrae). Ectopic calcification, particu-larly in the falx ceribri, is present in more than 90% of affected individuals, cardiac and ovarian fibromas occur in approximately 2% and 20% of individuals respectively. Approximately 5% of children with GGS develop medul-loblastoma [6].
The prevalence of Gorlin syndrome varies from one coun-try to another. 1: 55,600 in England, [7] in Australia it was 1:1,64,000, [8] 1 :13,939,393 in Korea, [9] 1:2,56,000 in Italy. [10] The frequency of the NBCCS has been variously estimated, but there is more or less general agreement that the prevalence is about 1:60,000. [11] Gorlin syndrome is caused by germ-line mutations of the PTCH gene. [4] The human homolog of the Drosophila segment polarity gene Patched (PTCH) located in the 9q22.3-9q31 chromo-some is responsible for the development of GGS. [5]
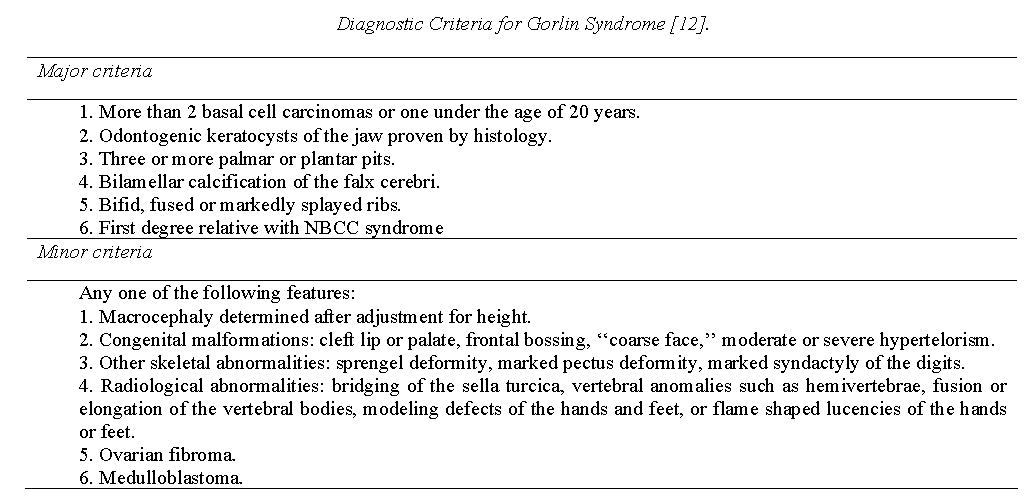
Gorlin Goltz syndrome is diagnosed in individuals with two major criteria and one minor criterion or one major and three minor criteria (Evans et al).[1] Kimonis et al [12] modified Evans criteria to include more minor criterias.
Since the syndrome is a hereditary condition, thus referral to a geneticist for counselling is mandatory. It is recom-mended to involve families in regular screening. It may be possible to prove whether someone in a family has inherited the condition or not by DNA tests, either by tracking the chromosome 9 containing the faulty gene, or by direct analysis of the mutation causing the disease in a particular family.
In our case, patient had three major criterias such as mul-tiple odontogenic keratocysts, bifid rib and multiple Nevi and hence it was diagnosed as Gorlin Goltz syndrome.
Early diagnosis of the syndrome is essential to treat it effectively and thereby minimising the complications. Interdisciplinary cooperation of oral and maxillofacial surgeons, oral pathologists, paediatricians, dermatolo-gists, and specialists in genetics is mandatory in the diag-nosis, treatment and follow-up of patients with Gorlin Goltz syndrome.
References
- Evans DGR, ladusans EJ, Rimmer S, Burnell LD, Thakker N, Farndon PA. Complications of the nevoid basal cell carcinoma syndrome: results of a population based study. J Med Genet 1993;30:460-464.
- Fitzpatrick PJ, Thompson GA: Gorlin's syndrome, or nevoid basal cell carcinoma syndrome. Can Med Assoc J 1982; 127: 465-470.
- Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epi-thelioma, jaw cyst and bifid rib: A syndrome. New Engl J Med 1960; 5: 204-210.
- Gu XM, Zhao HS, Sun LS, Li TJ. PTCH mutations in sporadic and Gorlin-syndrome-related odontogenic keratocysts. J Dent Res 2006; 85(9): 859-863.
- Johnson RL, Rothman AL, Xie J, Goodrich LV, Bare JW, Bonifas JM et al. Human homolog of patched, a candidate gene for the basal cell nevus syndrome. Sci-ence 1996; 272: 1668-16671.
- Evans DG, Farndon PA. Nevoid Basal Cell Carcinoma Syndrome. Gene Reviews 2008. (cited on 2010 Jan 14) Available from: URL: http://www.ncbi.nlm.nih. gov/ bookshelf/br.fcgi?book=gene&part=bcns.
- Evans DG, Farndon PA, Burnell LD, Gattamaneni HR, Birch JM. The incidence of Gorlin syndrome in 173 consecutive cases of medulloblastoma. Br J Cancer 1991; 64 (5): 959-961.
- Shanley S, Ratcliffe J, Hockey A, Haan E, Oley C, Ra-vine D et al. Nevoid basal cell carcinoma syndrome: review of 118 affected individuals. Am J Med Genet 1994; 15: 50 (3):282-290.
- Ahn SG, Lim YS, Kim DK, Kim SG, Lee SH, Yoon JH. Nevoid basal cell carcinoma syndrome: a retrospec-tive analysis of 33 affected Korean individuals. Int J Oral Maxillofac Surg 2004; 33(5): 458-462.
- Lo Muzio L, Nocini PF, Savoia A, Consolo U, Procac-cini M, Zelante L et al. Nevoid basal cell carcinoma syndrome. Clinical findings in 37 Italian affected indi-viduals. Clin Genet 1999; 55 (1): 34-40.
- Gorlin RJ. Nevoid basal cell carcinoma (Gorlin) syn-drome: unanswered issues. J Lab Clin Med 1999 ;134 (6): 551-552.
- Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, DiGiovanna JJ et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syn-drome. Am J Med Genet 1997; 31; 69(3): 299-308.